|

|
|
The Meninges and Tarlovcysts
The Meninges
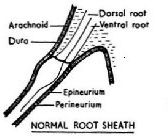
'The spinal meninges are subdivided as the dura, arachnoid, and pia mater and are the connectivetissue membranes that surround and support the spinal cord and cauda equina. The outermost of the meninges is the dura mater, which is fibrous and tough and is anchored to the periosteum at the foramen magnum. The dura mater extends inferiorly to the sacrum. The extradural or epidural space (between dura mater and vertebral periosteum) contains fat, loose connective tissue, and venous plexuses. The arachnoid matter is the more delicate, membranous intermediate tissue that follows the dura inferiorly to S2 and laterally to intervertebral foramina. The subdural space, between dura mater and arachnoid mater, contains only a film of lubricating cerebrospinal fluid (CSF). The pia mater is the innermost membranous covering that adheres closely to the surface of the spinal cord, enclosing networks of blood vessels. The subarachnoid space, located between the arachnoid mater and the pia mater, contains CSF. Within the dural sac inferior to the termination of the spinal cord, the subarachnoid space contains the cauda equina and filum terminale. Tumors of the spinal cord account for 15f all CNS tumors, with an incidence of 0.5 to 2.5 cases per 100,000 population. Spinal tumors are divided into extradural, intradural-extramedullary, and intradural- intramedullary. Extradural tumors make up 50f all spinal tumors, while intradural extramedullary tumors account for 40and intraduralintramedullary tumors account for 5 to 10Extradural masses are most often metastatic lesions arising from the vertebral bodies. Intradural-intramedullary neoplasms arise from the spinal cord itself and are typically characterized by expansion of the cord. Intradural-extramedullary masses originate within the dura but outside the actual spinalcord and are located within the subarachnoid space
Tarlov Cysts
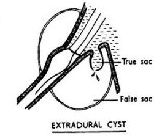
Tarlov cysts exist because of a weakness in the meninges, which results in the arachnoid membrane being pushed through a weak point in the dura.
Back ground
Tarlov Cyst
November, 2006
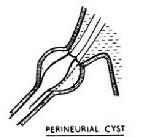
Tarlov cysts are fluid-filled nerve root cysts found most commonly at the sacral level of the spine the vertebrae at the base of the spine. These cysts typically occur along the posterior nerve roots. Cysts can be valved or nonvalved. The main feature that distinguishes Tarlov cysts from other spinal lesions is the presence of spinal nerve root fibers within the cyst wall, or in the cyst cavity itself.
Due to the close proximity to the lower pelvic region, patients may be misdiagnosed with herniated lumbar discs, arachnoiditis, and in females, gynecological conditions. An accurate diagnosis may be further complicated if the patient has another condition that affects the same region.
Incidence and Prevalence
Small, asymptomatic Tarlov cysts are actually present in an estimated 5 to 9 percent of the general population. However, large cysts that cause symptoms are relatively rare. Tarlov cysts were first identified in 1938, yet there is still very limited scientific knowledge available.
In a recent Tarlov cyst survey, an estimated 86.6 percent of respondents were female, and 13.4 percent were male. This condition affects women far more frequently than it affects men. The largest majority of respondents were ages 31 to 60, with a combined total of 80.4 percent in that age demographic.
An estimated 33 percent of respondents had a cyst(s) present in other parts of the body, most commonly the abdomen or hand and wrists.
An estimated 3 percent of respondents had no pain; 4.2 percent categorized their pain as very mild; 7.6 percent as mild; 31.5 percent as moderate; 38.6 percent as severe; and 15.1 percent as very severe.
Source:
Tarlov Cyst Support Group, Tarlov Cyst Survey
Causes
Although the exact cause is unknown, there are theories as to what may cause an asymptomatic Tarlov cyst to produce symptoms. In several documented cases, accidents or falls involving the tailbone area of the spine caused previously undiagnosed Tarlov cysts to flare up.
Symptoms
An increase in pressure in or on the cysts may increase symptoms and cause nerve damage. Sitting, standing, walking, and bending are typically painful, and often, the only position that provides relief, is reclining flat on ones side. Symptoms vary greatly by patient, and may flare up and then subside. Any of the following may be present in patients that have symptomatic Tarlov cysts.
* Pain in the area of the nerves affected by the cysts, especially the buttocks
* Weakness of muscles
* Difficulty sitting for prolonged periods
* Loss of sensation on the skin
* Loss of reflexes
* Changes in bowel function such as constipation
* Changes in bladder function including increased frequency or incontinence
* Changes in sexual function
Diagnosis
Tarlov cyst is difficult to diagnose because of the limited knowledge about the condition, and because many of the symptoms can mimic other disorders. Most primary care physicians would not consider the possibility of Tarlov cyst. It is best to consult a neurosurgeon with experience in treating this condition.
Tarlov cysts may be discovered when patients with low back pain or sciatica have a magnetic resonance imaging (MRI) performed. Follow-up radiological studies, in particular, computed tomographic (CT) myelography are usually recommended.
If a patient has bladder problems and seeks medical help from an urologist, there are tests that can help diagnose Tarlov cyst. The standard urological tests for Tarlov cyst help determine if the patient has a neurogenic (malfunctioning) bladder. In urodynamics, the bladder is filled with water through a catheter and the responses are noted. Cystoscopy involves inserting a tube with a miniature video camera into the bladder via the urethra. A neurogenic bladder shows excessive muscularity. A third possible test is a kidney ultrasound to see if urine is backing up into the kidneys.
Nonsurgical Treatment
Nonsurgical therapies include lumbar drainage of the cerebrospinal fluid (CSF), CT scanning-guided cyst aspiration, and a newer technique involving removing the CSF from inside the cyst and then filling the space with a fibrin glue injection. Unfortunately, none of these procedures prevent symptomatic cyst recurrence.
Surgery
Tarlov cyst surgery involves exposing the region of the spine where the cyst is located. The cyst is opened and the fluid drained, and then in order to prevent the fluid from returning, the cyst is occluded with a fibrin glue injection or other matter.
Neurosurgical techniques for symptomatic Tarlov cysts include simple decompressive laminectomy, cyst and/or nerve root excision, and microsurgical cyst fenestration and imbrication.
The authors of one study found that patients with Tarlov cysts larger than 1.5 cm and with associated radicular pain or bowel/bladder dysfunction benefited most from surgery. The benefits of surgery should always be weighed carefully against its risks.
Outcome
Postoperative CSF leak is the most common complication, but in some cases, these leaks may self-heal. Patients may be advised to stay in bed with the foot of the bed raised, and to wear a corset to control swelling. Although it is low, there is a risk of developing bacterial meningitis. Although some patients have noted a considerable decrease in pain, the most common negative outcome is the failure of the surgery to eliminate the symptoms. In some cases, the surgery may cause an existing symptom to worsen or it may cause a new one.
When all treatment options have been exhausted, it is very important for the patient to make any necessary lifestyle changes and to undertake a pain management strategy with his or her physician. Supervised pain management, as well as support groups, can help a patient cope and improve his or her quality of life.
Tarlov Cyst Resources
Tarlov Cyst Association
|
|
