|
All About Arachnoïd cysts on MRI pictures
KYSTES MENINGES RACHIDIENS (summary)
- Called arachnoïd cysts, perineural Tarlov cysts, lepto-meningeal cysts,
- They are meningeal diverticulae that are communicating (most of them) with the sub-arachnoïdian space.
- Most are extral-dural arachnoïd cysts, but some are intra-dural ones. Very few are both extra and intra dural.
- Most of arachnoïd cysts are congenital or idiopathic, but some develop after a trauma, a surgery, a myelography, saccoradiculography with pantopaque as contrast medium, infection, sub-arachnoïdian haemorrhage, or an epidural anaesthesia
Symptoms depend on the size and the location of the cyst.
Most of them are not symptomatic, but for some, there are signs or symptoms of radicullar (nerve root) or medullar compression.
Arachnoïd cysts at the neck and dorsal level can give sensitive problems like hypoesthesia (1/3) with spasticity in the inferior part of the body (legs) for 2/3 of cases.
Those located in the lumbar and sacral part of the body can be the cause for a radiculopathy (nerve roots pain) with lombalgia and radicular pain in the butt, pelvis and/or leg area, sphincterian troubles
.
Symptoms can change with the position as in the standing position they could be more important due to the filling of the cyst.
Cervical and dorsal cysts are found for nearly all cases in teens,
Lumbar and sacral are found in adults.
Neuroradiologist point of view
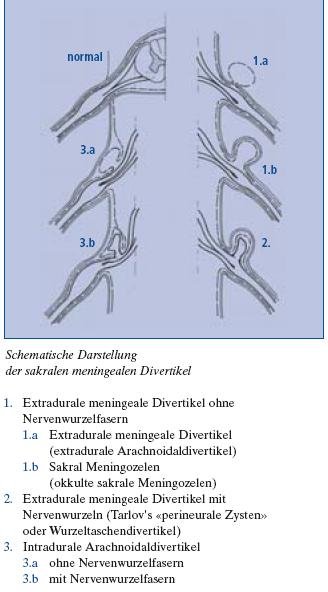
Nabors and al classified Arachnoïd cysts according to three types:
- Type I : extra-dural, no nerve roots or rootlets such as intra-sacral méningocèles, probably from congenital origin, that develop from the dural bag to which they are connected by a little collar. They are found at the very place where a dorsal nerve root comes out the dural bag. They are sometimes difficult to be precisely identified and can be seen as a type II cyst on pictures. These ones are often associated with some foramina hole enlargement, and with a scalloping of the vertebrae. It is very important to distinguish them from the sacral meningocelaes going to the pelvis area et very often associated with other congenital abnormalities ( teratomes, dermoïdes, lipomes, and other abnormalities( uro-genital and ano-rectal)
- Type II: Extra-dural with a nerve root inside (such as Tarlov or perineural cysts). There are very often not only one but multiple and mostly found in the sacrum area. There are of two kinds: Tarlov (perineural) cysts are after the posterior root ganglion, with nerve fibres inside or nerve tissue in the walls, they are not communicating with the perineural arachnoïdian space. They normally are very small in the upper rachidian part, but can be bigger (to 3cm) when located in the lower part of the sacrum. The second kind in this type is meningeal diverticulaes. They are located before the nerve root ganglion, with nerves fibres inside and are largely communicating with the subarachnoïdian space. 75f all extra dural cysts (except for Tarlov cysts) are located in the thoracic area, 20n the lumbar and sacral area, and 5n the cervical area. Most of them are located behind or on the side of the dural bag. 50an spread towards the foramina hole. They are large, communicating with subarachnoïdian spaces, and can be large enough to extend to 6 vertebrae levels. There is bone erosion in the foramina hole, or rachidian canal with enlargement for most of extra dural cysts.
- Type III: intra-dural, congenital or made because of traumas
and are rarely associated with other abnormalities. They are very rare. 75re found in the dorsal area. Most of the congenital ones are located behind the spinal cord on the contrary of those happening because of a trauma
that mostly are located anterior to the spinal cord.
On MRI pictures, the signal is the same as the CSF one.
If MRI made with a contrast medium:
- The signal in the cyst is the same as in the dural bag.
- The signal for cysts due to traumas
is a little stronger at the periphery or nerve root location
- The signal is more important for other causes: synovial cysts, dermoïdes or épidermoïdes cysts, teratomes
From : Imagerie par Résonnance Magnétique de la Tête et du rachis »
Case 87,93 : kystes méningés rachidiens, pages 684 et 685
Par Jean Claude Tamraz, C. Outin, M. Forjaz Secca - 2004 - Medical - 717 pages
Editeur : Springer Verlag
Principes d'imagerie par résonance magnétique de la tête, de la base du crâne et du rachis
Approche anatomo-clinique et guide d'interprétation
Tamraz, J., Outin, C., Forjaz Secca, M., Soussi, B.
2ieme ed. revue et augmentée, 2004, XII, 717 p., Broché
ISBN: 978-2-287-59742-8
|
